Implementation and Evaluation of Walking Groups with Older Women in Rural Communities: A Pilot Project
Implementation and Evaluation of Walking Groups with Older Women in Rural Communities: A Pilot Project
Elaine Bowen
Nancy O’Hara Tompkins
Judy Matlick
Rebecca Mowbray Smith
West Virginia University
Shannon Holland
West Virginia Arthritis Foundation
Abstract:
Low-income, older rural women are least likely to meet physical activity recommendations and are at increased chronic disease risk. Women involved in an established community organization provided leadership for a social support–based walking group. Leaders received an information kit for a six-week walking challenge and recruited individuals. Leaders and individuals met on average 4.7 times to support the program. Weekly step logs, as well as surveys of individuals and group leaders, were analyzed with these results: (1) significant walking increases over six weeks; (2) 86.7 percent of individuals intended to continue walking; and (3) 66.7 percent of leaders were between ages 50 and 69, with 24 percent between ages 70 and 89. Based on this experience, other physical activity promotions may have similar success by partnering with existing civic organizations and developing a volunteer leader network with older women.
Key words
Exercise, health promotion, older adults, organizational case studies, partnerships, physical activity, prevention of chronic disease, rural health, state and community programs, women’s health
Introduction
Background
Despite the known benefits of physical activity for decreasing the risk of chronic diseases, more than two-thirds of American adults do not meet recommended levels of physical activity (Centers for Disease Control and Prevention 2001). Among women, those who are older and live in rural areas have a lower income and are least likely to meet physical activity recommendations. This poses an increased risk for chronic disease (Haskell, I-Min et al. 2007; Parks, Housemann, and Brownson 2003). Women in West Virginia fare particularly poorly on a number of chronic disease indicators (National Women’s Law Center 2010); compared to women in other states and U.S. territories, women in West Virginia ranked 49thfor high blood pressure (36.3 percent), 51st for diabetes (12.9 percent), 48th for obesity (32.6 percent), and 51st for no leisure time physical activity (36.8 percent). Rye et al. found a lack of support and willpower to be the dominant barriers to physical activity among low-income women in West Virginia (Rye et al. 2009). Evidence-based social support interventions to increase physical activity are highly recommended (Centers for Disease Control and Prevention 2010); they typically focus on building, strengthening, or maintaining social networks that provide support for behavior change (e.g., setting up a buddy system, setting up walking groups to provide friendship and support). West Virginia’s plan to improve physical activity and nutrition recommends use of social support interventions to increase physical activity (West Virginia Department of Health and Human Resources n.d.).
This project took place in a largely rural state. Sixty-four percent of West Virginia’s population lives in communities of less than 2,500 people, and the U.S. Census Bureau has designated 45 of its 55 counties as “nonmetropolitan” (Bellamy et al. 2003). West Virginia’s rural communities exemplify those described by Phillips and McLeroy (2004), as having population dispersion, low socioeconomic status, transportation challenges, and minimal public funding for recreational facilities and programs.
This paper describes the implementation and evaluation of a community-based social support intervention to increase physical activity among women in West Virginia. Delivered through the Community Educational Outreach Service (CEOS), a statewide community-based education and civic organization, the program was titled CEOS on the Move. Implementation and evaluation of CEOS on the Move occurred under “real world” conditions, including a limited budget and use of volunteers, as described by Chan and Tudor-Locke (2008). CEOS volunteers agreed to recruit individuals, conduct weekly group sessions, and coordinate data collection. The West Virginia University Extension Service and West Virginia on the Move, Inc., a nonprofit organization with a mission to promote a physically active lifestyle for the prevention of chronic disease, provided oversight for program implementation and evaluation.
CEOS originated in 1914 as Farm Women’s Clubs and has partnered with West Virginia University Extension Service since that time. This project was the first time that West Virginia on the Move partnered with either organization. Statewide, CEOS has approximately 271 clubs with 4,400 members in 45 of the 55 counties. Members are typically older adult women living in rural communities. Clubs meet monthly and feature a healthy lifestyle activity led by a member who volunteers to be the club Health Motivator.
A survey of CEOS members conducted in 2008-2009 indicated that walking was the most common form of physical activity for club members (Bowen, Matlick, and Mowbray 2010). The goal of CEOS on the Move was to expand current efforts to increase physical activity levels of individuals and to strengthen the leadership capacity of CEOS clubs to promote chronic disease prevention initiatives in their communities. Because CEOS clubs were already an established social nucleus within their communities, this project aimed to impact the physical activity levels of individuals, groups, and the community at large through CEOS’s reach.
Walking kits and recruitment of leaders and individuals
In February 2010, walking group kits were developed by West Virginia University Extension Service and West Virginia on the Move. The project team reviewed several existing walking guides and materials, and sought input from CEOS leaders to create the walking kit content and format. Kits contained the following:
- a leader training outline
- walking group leader’s guide and weekly step total chart
- participant’s guide and walking log
- evaluation survey
- news article and proclamation
- emergency health form
- two participant handout templates and
- Sportline 330 pedometers.
Timeline
March 2010 — CEOS club presidents were mailed an invitation requesting their help in identifying leaders to start a walking group in their community. Clubs were encouraged to recruit walking group participants from among their existing club members, as well as family, friends, and neighbors. Any CEOS member, including Health Motivators, could volunteer to be a walking group leader. Each leader who completed an application listing walking group members received a free kit. The pedometers provided were simple step-counters deemed to be of acceptable quality, and each group leader received additional ones in case any failed.
April-May 2010 — Local trainings were conducted by county Extension agents to familiarize leaders with the project, kit contents, and reporting procedures. Following the leader training, walking groups began a six-week walking challenge. Walking group leaders conducted weekly interactive sessions about health, walking, reducing calories, increasing steps, and setting goals. Individuals learned to use a pedometer and reported weekly steps. Three weeks into the challenge, walking group leaders were sent postcards thanking them for their leadership and reminding them to send the surveys and logs at the end of the challenge.
Evaluation methods
Evaluation was at multiple levels and used four data collection methods and sources: (1) program adoption and reach; (2) individual weekly step totals; (3) individual surveys; and (4) group leader surveys.
- Program adoption and reach were calculated at the county, CEOS club, and individual levels, using aspects of the RE-AIM method used in other physical activity evaluations (Bopp et al. 2010). The number of eligible settings (county and club) and individuals was divided by the number actually participating.
- Individuals’ walking step totals were collected weekly for six weeks and tabulated by the group leader.
- A 20-item post-survey developed by the project team was distributed to individuals by the group leaders at the end of the six-week challenge. As an incentive, each group that returned any completed surveys received an exercise DVD. In addition to demographic information, the survey included questions pertaining to individuals’ perceptions of the usefulness of walking kit components, their motivations for joining the walking group, their intentions to continue walking, barriers to continuing to walk, and personal benefits they attributed to walking group participation.
- One month following the end of the six-week group challenge, a sixteen-item survey was mailed to leaders. Survey items included the following: number of individuals who signed up for the walking group; number of CEOS members and nonmembers; group meeting frequency; participation in weekly meetings; leader use of the kit materials; other community group partnerships; problems and successes; interest in future walking challenges; personal benefits from the walking group; age; and whether they were a club Health Motivator.
To assess the project’s success, the project team reviewed the quantitative and qualitative survey data as well as informal feedback from the partner organizations. In October 2010, a summary of the results of the walking group challenge and surveys was presented to CEOS leaders, walking group leaders, the West Virginia University Extension Service, and West Virginia on the Move.
West Virginia on the Move supported the project with funding from the Benedum Foundation. Significant in-kind resources were provided by West Virginia University Extension Service. The evaluation protocol was approved by the University’s Institutional Review Board.
Evaluation results
| Level of Evaluation | Potential reach | Actual adoption and reach | Response rates |
| County level | 45 counties had CEOS clubs | Walking groups were formed in 26 counties (57.8 percent of total counties) | Walking group leaders in 19 counties returned surveys (73 percent of total counties represented) |
| Club level | 271 CEOS clubs were located in the 45 counties | 59 CEOS clubs formed a walking group (21.8 percent of total clubs) | 49 walking group leaders returned 6-week step totals (83.0 percent of 59 groups); 34 walking group leaders returned completed surveys (57.6 percent of 59 groups) |
| Individual level | There were 4,400 CEOS club members in the 271 clubs located in 45 counties | 766 individuals joined a walking group; approximately 398 of these were CEOS club members (9 percent of total statewide membership) | 244 individuals reported 6-week step totals (31.9 percent of 766 individuals) 380 individuals returned completed surveys (49.6 percent of total 766 individuals) |
Table 1. Program adoption, reach, and response rates.
Program adoption and reach. Using the RE-AIM framework, the number of eligible settings (club and county) and individuals was divided by the number actually participating. There were 59 groups initiated and led by CEOS members. Considering the total of 271 clubs in West Virginia, the 59 groups represent a club response rate to recruitment of 21.8 percent. Among the 45 counties with CEOS clubs, walking groups were formed in 26 counties, yielding a county adoption rate of 57.8 percent. The club and county adoption rates were calculated to identify opportunities for increased walking group participation and guide future recruitment efforts. Group applications at the beginning of the walking challenge listed 766 total individuals, an average of 12 per group. Based on the leader survey responses, an estimated 398 CEOS club members participated in the walking groups. This is about nine percent of the total statewide CEOS target population of 4,400 members. The remaining 368 walking group individuals were CEOS friends, family, or other individuals from the community. Dropout and completion rates were not monitored. Therefore, it is not known how many maintained participation or the reasons why some individuals did not return their survey.
Individual weekly step totals. Leaders collected weekly step totals reported by their group individuals (see Figure 1). Forty-nine leaders (83.0 percent) returned charts with 244 individuals who reported step totals for all six weeks. Figure 1 shows a trend of increasing steps, with the greatest step increases in weeks three and six.
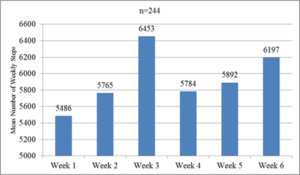
Figure 1. Step totals reported weekly by individuals to group leaders.
Individual survey findings. Leaders returned completed surveys from 380 individuals. This was a 49.6 percent return rate. Individuals were primarily female (87.1 percent). Their ages ranged from 30 years and under to 90 and over, with almost half (49.7 percent) in the 50 to 69 age range and more than a fourth (27.5 percent) in the 70 to 89 age range. Most individuals rated their health as good (52.7 percent) or satisfactory (29.7 percent). Individuals were asked how many steps they logged in the first week and also in the sixth week. Over the six-week period, steps increased by a mean of 4,342 or 724 per week. A paired samples t-test revealed a statistically significant difference between the mean number of total steps in the first week and the mean number of total steps in the last week. This is consistent with the steps reported weekly to the leaders, as shown in Figure 1.
Individuals were also asked how often they walked for exercise before joining the walking group and since joining the group (see Figure 2). The Wilcoxon Matched-Pairs Signed-Ranks Test was significant (p<.0001) with positive pre-post differences for 203 individuals. Responses for less than once a week decreased from 37.1 percent before joining to 12.4 percent after joining. Likewise, 61.1 percent walked at least one time a week before joining the walking group, and 85.0 percent of individuals walked at least one time a week after joining the group. It is notable that some individuals, 14.3 percent, said they did not record their walking steps. This may account for the lower number of individuals who reported weekly step totals to their group leader.
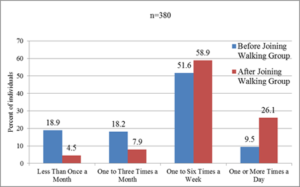
Figure 2. Comparisons of self-reported walking before and after joining the group.
When asked if they would rather walk in a group or by themselves, 45.1 percent reported they would rather walk by themselves and 54.9 percent would rather walk in a group. As shown in Figure 3, individuals reported a variety of locations for their group walks, and the predominant location was their neighborhood.

Figure 3. A variety of locations for group walking activity was reported.
The main motivations to join a walking group were reported as (1) more physical activity (62.1 percent); (2) knew other individuals (49.5 percent); (3) sounded enjoyable (41.8 percent); (4) weight loss (39.2 percent); (5) told by doctor to exercise (24.2 percent); and (6) guilt about not exercising enough (22.1 percent).
In an open-ended format, individuals reported that their primary barriers for walking regularly were weather, health/illness, and being busy/lack of time. The top three self-reported benefits from the walking group were felt better, lost weight, and more exercise/energy. Individuals rated the following items in order of most useful to least useful: walking log; pedometer; walking guide; social time with other walkers; and weekly meeting. Individuals also suggested the following program improvements: a better pedometer; include ideas for individual walkers; coordination of schedules and walking times; more ways to keep people motivated; and the addition of nutrition information. Nearly 87 percent of respondents planned to continue walking after the challenge. When asked if the walking group program should continue year-round, 65.1 percent reported yes, 29.4 percent were unsure, and 5.4 percent reported no.
Group leader survey findings. Follow-up surveys were completed and returned by 34 walking group leaders. This was a 57.6 percent return rate, as noted in Table 1. The majority of the leaders (66.7 percent) were in the 50 to 69 age group. Twenty-four percent of the leaders were between the ages of 70 and 89. Nine percent were in the 30 to 49 age group. Most walking group leaders (54.5 percent) were not club Health Motivators. Leaders estimated that 52 percent of the individuals were CEOS members. Groups met an average of 4.7 times during the six-week challenge, with an average of 5.5 individuals attending the scheduled meetings. This was approximately 43 percent of the group membership. Twenty-one percent reported always using the leader’s guide in their weekly meetings, 54.5 percent sometimes used the guide, and 24.2 percent never used the guide. Some leaders (12.1 percent) partnered with other community organizations, such as the health department, library, and Take Off Pounds Sensibly (TOPS). Nearly all of the leaders cited gaining at least one personal benefit from the walking group. The most common benefits cited were feeling better and enjoying time with others. Most leaders (66.7 percent) were interested in getting walking group information in the future, although 24.2 percent were unsure, and 9.1 percent were not interested.
Walking group leaders reported problems in scheduling group meetings and getting individuals to attend regularly. Individuals’ physical limitations and inclement weather posed additional difficulties for the leaders. Twenty-six leaders cited group successes, such as starting a weekly Zumba class and recruiting new CEOS club members. Individual successes included continued walking, improving blood pressure, controlling diabetes, losing weight, and having fun.
Interpretation
The walking program was successful in promoting physical activity in rural communities. Partnering with West Virginia on the Move enhanced the credibility and overall impact of the project, reaching CEOS club members and the greater community. The formation of 59 walking groups indicated a strong need for and interest in community walking groups. The walking groups were built on the existing CEOS organizational structure, so it was not necessary to develop a new system for communication and recruitment. CEOS club members often live in or near the same community, which seemed to make it convenient for members to join a walking group, walk together, and communicate. Club members recruited family members, friends, and other community residents to join their walking groups, as evidenced by the fact that 48 percent of individuals were non-CEOS club members. The non-CEOS members who participated were under no obligation to join the organization in order to be in the walking groups. CEOS clubs have a reputation of being trusted in their communities, and this was likely to have had a positive impact on group formation and participation. Individuals may also have been enticed to join, because there were no costs involved and they received a free pedometer.
Survey responses revealed the complexity of social support, motivation, and group cohesion. It appeared that social support was generally helpful in recruiting individuals and fostering a sense of accountability to walk and log steps. Nearly half the individuals reported that they joined a group primarily because they knew others in the group. While 29 percent reported that the weekly meetings were not useful, 91 percent rated social time with other walkers as somewhat useful (28 percent) or very useful (63 percent). Because some individuals preferred to walk by themselves and regular meetings were a challenge for leaders, the project team concluded that the type and amount of social support needed is highly individual. It certainly requires more than six weeks to develop group relationships and walking habits. Further study is needed to provide clearer guidance on effective social support strategies to initiate and maintain walking groups.
Regarding the findings on individual step totals, it was not surprising that the mean step counts at the beginning of the walking campaign (5,485 steps/day) indicate that this older population was relatively inactive. Sherman at al. (2006) reported baseline step counts of 6,337 for rural women (average age 42 years), with an increase to 8,910 after a six-month primary care–based intervention. Warren at al. (2010) reported baseline steps a day of 5,839 for rural women participating in a worksite intervention. Women in the Warren study’s ten-week intervention increased their steps to 7,915 a day. Compared to other studies with rural women, individuals in this study reported fewer steps both at baseline and after six weeks, underscoring the need for physical activity programming and support.
Many of the CEOS clubs involved in the walking program have had a Health Motivator and received health messages regularly for several years. Fifty-five percent of the leaders reported they were not a club Health Motivator. Therefore, new leaders emerged from the opportunity for clubs to initiate a community walking group. Older women appeared to be a natural source for engaging others, as close to a fourth of both the walking group leaders and individuals were over 70 years old.
The project team encountered some challenges. Group leaders and individuals reported frustration with some pedometer failures. Another issue was that program survey response rates from both leaders and individuals were not as high as anticipated. Email and web surveys were not used because many individuals lacked broadband Internet access. Although response rates were lower than desired, they were higher than those reported by Chan and Tudor-Locke (2008) in their evaluation of a community-based pedometer intervention. Additional limitations to this study include selection, self-report, and social desirability biases. The reason for the spike in week three step totals could not be discerned in the program evaluation because factors such as weather and other variables were not tracked.
Future plans
Results provided insight into future walking programs and walking kit improvements. A walking kit was created and renamed “Wild Wonderful Walking Groups” and a professional design team gave it a polished look. The kit contains the same basic components, with the exception of pedometers and specific dates for a six-week walking challenge. The new walking log allows individuals to track either steps or minutes of walking. Individuals are encouraged to purchase their own pedometers. Further revisions will also capture factors such as weather and community events that may influence walking behavior. The walking group leader evaluation will be revised to include a section about participation to assess this variable. The project team strives to balance the need for program evaluation for program improvement and dissemination purposes with the burden of data collection on leaders and individuals.
The project team deems that this was a successful collaboration and continues to expand its partnership in promoting walking statewide. A future goal is to engage nonparticipating CEOS clubs and expand to new community systems, including work sites, women’s clubs, and other civic organizations. In addition to expanding participation, the project team wishes to support group walking year-round, as well as to incorporate more motivational strategies for group leaders and individuals.
In summary, forming social support-based walking groups through established networks of rural older women may influence health and chronic disease outcomes for this demographic, as well as for those within their sphere of social influence. This project also provides preliminary support for uncovering the untapped role of older rural women as physically active role models and change agents in their communities.
References
Bellamy, G., K. Stone, S. Richardson, and R. Goldsteen. 2003. “Getting from here to there: Evaluating West Virginia’s rural nonemergency medical transportation program.” Journal of Rural Health Supplement 19(5): 397-406.
Bopp, M., S. Wilcox, S. Hooker, S. Butler, L. McClorin, and M. Laken et al. 2007. “Using the RE-AIM framework to evaluate a physical activity intervention in churches.” Preventing Chronic Disease 4(4). http://www.cdc.gov/pcd/issues/2007/oct/06_0155.htm. Accessed February 18, 2014.
Bowen, E., J. Matlick, and R. Mowbray. 2010. “Health motivators on the move: Partnerships and social support systems.” Journal of the National Extension Association of Family and Consumer Sciences 5: 1-10.
Centers for Disease Control and Prevention. 2007. “Prevalence of regular physical activity among adults—United States, 2001and 2005.” Morbidity and Mortality Weekly Report (MMWR) 56: 1209-1212.
Centers for Disease Control and Prevention. 2010. Behavioral and social approaches to increase physical activity: Social support interventions in community settings. http://www.thecomunityguide.org/pa/behavioral-social/community.html. Accessed February 18, 2014.
Chan, C. B., and C. Tudor-Locke. 2008. “Real world evaluation of a community-based pedometer intervention.” Journal of Physical Activity Health 5: 648-664.
Haskell, W. L., L. I-Min, R. R. Pate, K. E. Powell, S. N. Blair, and B. A. Franklin, et al. 2007. “Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association.” http://circ.ahajournals.org/. Accessed February 18, 2014.
National Women’s Law Center. 2010. “Making the grade on women’s health: A national and state-by-state report card.” http://hrc.nwlc.org/states/west virginia. Accessed April 7, 2013.
Parks, S. E., R. A. Housemann, and R. C. Brownson. 2003. “Differential correlates of physical activity in urban and rural adults of various socioeconomic backgrounds in the United States.” Journal of Epidemiology and Community Health 57: 29-35.
Phillips, C. D., and K. R. McLeroy. 2004. “Tailoring programs and services to meet rural needs.” American Journal of Public Health 94(10): 1662-1663.
Rye, J., S. Rye, I. Tessaro, and J. Coffindaffer. 2009. “Perceived barriers to physical activity according to stage of change and body mass index in the state WISEWOMAN population.” Women’s Health Issues 19: 126-134.
Sherman, B. J., G. Gilliland, J. L. Speckman, and K. M. Freund. 2007. “The effect of a primary care exercise intervention for rural women.” Preventive Medicine 44: 198-201.
Warren, B. S., M. Maley, L. J. Sugarwala, M. T. Well, and C. M. Devine. 2010. “Small steps are easier together: A goal-based ecological intervention to increase walking by women in rural worksites.” Preventive Medicine 50: 230-234
West Virginia Department of Health and Human Resources. N.d. West Virginia Bureau for Public Health. West Virginia everyday: A state plan to improve physical activity and nutrition.
http://www.ncsu.edu/ffci/publications/2014/v19-n2-2014-fall/index-v19-n2-december-2014.php
Back to table of contents ->https://www.theforumjournal.org/2017/08/30/fall-2014-vol-19-no-2/